
My colleague
Eli Perencevich wrote an
interesting blog this week in which he discusses airport screening. He points out that some of the discussion surrounding travel restrictions and Ebola are related to ideas from (and models of) epidemics of respiratory viruses, including the 2009 H1N1 pandemic. In the post he highlights some of the important differences between Ebola and influenza:
. . . Ebola is slower moving, has a much longer incubation period (especially compared to the duration of a transcontinental flight), and is not contagious before symptoms develop. What does this mean? It means that if Ebola was as infectious as influenza, millions would have already died - apocalypse. It also means that since Ebola is not transmissible during its long incubation period, it may be possible to quickly isolate patients when symptoms develop. Thus, airport screening on exit or entry could limit transmission and perhaps through early diagnosis allow Ebola infected patients to receive life saving treatment more quickly.
Later in the post he highlights the need for mathematical model-based analysis of the impact of specific Ebola screening programs. I recommend reading the blog.
As I mentioned in a comment to the piece, in addition to incubation period, it's useful to consider the serial interval (the period between infection and transmission; sometimes also referred to as the
generation interval or
generation time) and basic reproduction ratio (
R0). As
discussed before, estimates for
R0 for Ebola in this event are similar to estimates of
R0 for pandemic influenza events.
White and Pagano estimate the serial interval for a 1995 outbreak of Ebola in Congo to be 5.4-7.6 days and the
WHO Ebola Response Team estimates the serial interval for the current epidemic to be near 15
days. By comparison,
estimates of the serial interval for the 2009 pandemic of influenza fall in the range of 2.5-3.0 days. Ebola has
much longer serial intervals than does influenza.
What do we take away from this? One thing is that the serial interval is important for understanding the
speed of spread. Perencevich observes that
. . . the first case of Ebola is thought to have occurred 307 days ago on December 6th in a two-year old boy. Since that time there have been an estimated 8,032 cases (granted these could be underestimates). If you compare a similar 307-day period for 2009 H1N1, April 12, 2009 to February 12, 2010 CDC estimated that between 42 million and 86 million cases occurred in the US with a mid-level estimate of 59 million people infected. Think about that -- 7,300 times more cases of H1N1 using the mid-level estimate during the same 307 days.
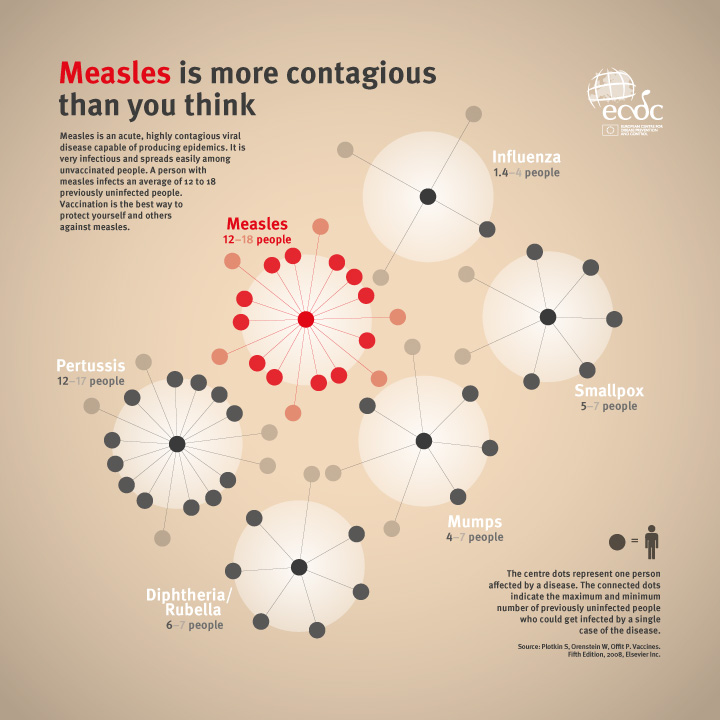
It's clear, then, that equating influenza and Ebola on the basis of
R0 alone is misleading. Thinking of
R0 as a reproductive factor for each generation of infection (at the beginning of an epidemic in a susceptible population) and the serial interval as how rapidly generations of infection occur, however, it becomes clearer that the much shorter serial interval of influenza is related the explosive emergence of influenza cases in 2009-10 relative to Ebola in 2013-14, despite the similar
R0 values. It's more complex than this in reality;
Wallinga and Lipsitch present a detailed mathematical treatment of how generation intervals shape the relationship between epidemic growth rates and reproductive numbers, and
Lipsitch et al illustrate, within the context of SARS, how incubation period, serial interval, and epidemic growth rate combine to produce estimates of
R0.
Another thing to ponder is that longer serial intervals can, depending on the length of the incubation period, give more time to institute control measures. On the one hand, the long serial interval relative to incubation period in the case of Ebola may suggest a higher likelihood of detecting an infectious traveler in an airport than there is for influenza. On the other hand, the extremely low incidence of Ebola in passengers must also be considered; it may not be an efficient activity to devote resources to.
I agree with Eli that mathematical
models can help shed light on such questions. Perhaps such models have been published, I admit to falling behind on the mathematical epidemiology of Ebola results in the last two weeks.
(image source: David Hartley)






.png)





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}