 The current outbreak of Ebola hemorrhagic fever in western Africa has been
ongoing for months. It is a remarkable and tragic event. Sadly,
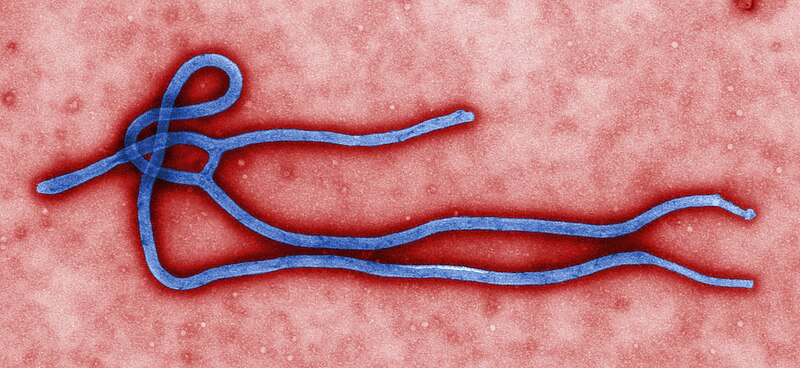
there is no known cure, the case fatality proportion is high (historically 50-90%), and
prevention is difficult in the areas where the virus is currently spreading.
The current outbreak of Ebola hemorrhagic fever in western Africa has been
ongoing for months. It is a remarkable and tragic event. Sadly,
there is no known cure, the case fatality proportion is high (historically 50-90%), and
prevention is difficult in the areas where the virus is currently spreading. be alert for signs and symptoms of EVD [Ebola virus disease] in patients with compatible illness who have a recent (within 21 days) travel history to countries where the outbreak is occurring, and should consider isolation of those patients meeting these criteria, pending diagnostic testing.Infection control procedures are standard and the necessary supplies are plentiful in Western hospitals, making it unlikely that an Ebola patient would cause secondary infections in healthcare settings.
Moreover, Ebola virus is much less transmissible than many other viruses. Measles virus, for example, has basic reproduction ratios in the range of 11-18, whereas those for Ebola have been estimated to be between 1-2. For comparison, the basic reproductive ratio for influenza is estimated to be 3-4, for rubella 6-7, and for chickenpox 10-12. The ratio for pertussis is similar to that of measles. One wonders what the basic reproduction ratio is for the current outbreak in Africa is (and if analytic approaches using social media might be helpful for estimating it).
Given that the current outbreak is so large compared to past outbreaks of Ebola, we might learn some lessons about this exotic disease. For example, are there transmission pathways that we don't know of at present? Aerosol transmission is thought to play only a minor role if any in transmission of human strains of Ebola virus, but perhaps new information will emerge from future epidemiological studies of the current outbreak.
{kind=link}
Dave, what is the relationship between reproductive ratios and transmission rates? Is that a one-to-one mapping? If you had asked me beforehand which was more likely to be "catchy," flu or measles, I'd've said flu every time. Mind you, I've had the flu, and no one I've known has had measles, so that probably colors my thinking on it - I'm guessing that's why we all get vaccinated against measles.
ReplyDeleteBiologically, the reproductive ratio is the number of cases caused by the first case of a disease when introduced into a completely susceptible population. If this quantity (known as "R0" in epidemiology) is greater than one, then the infection spreads; if it's less than one, then it doesn't. The greater R0 is above one, the more "explosive" epidemics tend to be. (Sometimes R0 is referred to as the "epidemic potential" for this reason.) R0 can depend upon many parameters; for many directly transmissible diseases, R0 is proportional to the adequate contact rate between individuals, but it also depends on other important quantities, including the period of infectiousness, the lifetime of individuals in the general population, and the disease-associated mortality rate. In the case of influenza and measles viruses, measles has a *much* higher R0 than that for influenza, and epidemics of measles in unvaccinated populations are notoriously explosive; see, e.g., the post http://musingsoninfection.blogspot.com/2014/04/measles-right-here-in-river-city.html and links therein for how problematic this disease is at present, even in the US. Ebola, thankfully, isn't aerosol infectious like measles is (see http://www.ncbi.nlm.nih.gov/pubmed/16916564 for a description of aerosol transmission in measles and similar infectious diseases). If it were, then the contact rate would be much higher and thus its R0 could be as well. (It should be noted that R0 isn't always as straight forward as described above as described in http://www.ncbi.nlm.nih.gov/pubmed/21860658, but it's often a helpful quantity to think about nonetheless.)
DeleteThank You for sharing this blog. Its very good to know the current status of Ebola Infection.
ReplyDeleteEbola Infection